Home
>
Blog
>
>
What Medical Malpractice Attorneys Should Follow Before Expert Record Review
- Use a medical narrative summary to organize the treatment story before the expert opens the full chart.
- Confirm whether the record set includes the key provider records.
- Flag missing records, unclear date ranges, and inconsistent documentation before the expert spends time reviewing.
- Keep the summary inside the records: organize and explain, but do not ask it to make conclusions.
- Give the expert a clear source trail so important points can be checked quickly against the chart.
Prepare the record before you prepare the expert
A medical narrative summary helps medical malpractice attorneys prepare for expert review by turning a complex chart into a clear, source-supported treatment story. The expert still reviews the records and forms the professional opinion, but the summary can reduce the time spent finding the basic sequence.
That matters in malpractice work.
The expert may need to review the admission history, provider notes, nursing documentation, medication records, operative reports, diagnostic studies, discharge instructions, and follow-up care. If those records arrive as a raw file stack, the first part of the expert review can become file reconstruction.
That is expensive time.
The goal before expert review is not to persuade the expert. It is to make the documented medical information easier to inspect, question, and verify.
Start with a clear expert-review purpose
Medical malpractice attorneys should define the review purpose before ordering or preparing a medical narrative summary.
An expert reviewing an emergency department timeline may need a different record focus than an expert reviewing surgical complications, delayed diagnosis questions, medication administration, postoperative monitoring, or discharge planning. A single generic summary may miss the reason the expert was retained.
Before expert review, clarify:
1. What period needs the closest review?
Name the admission, procedure, treatment window, office visit sequence, or post-discharge period that matters most.
2. Which specialties are involved?
A case involving emergency medicine, radiology, surgery, nursing, infectious disease, anesthesia, or primary care may need different record sections emphasized.
3. What records are expected?
List the records that should be present: facility chart, physician notes, nursing notes, medication administration records, labs, imaging, operative report, pathology, consent forms, discharge summary, and follow-up records.
4. What should be flagged, not concluded?
The summary can flag missing documents, timeline gaps, inconsistent histories, undocumented follow-up, or conflicting entries. It should not decide negligence, causation, liability, standard of care, or damages.
5. What format helps the expert work fastest?
Some experts prefer a narrative summary. Some need a chronology first. Some need both, with source references strong enough to move back into the chart quickly.
When this scope is clear, the medical narrative summary becomes more useful. It stops being a general report and starts becoming a structured handoff.
Need records prepared before expert review?
What breaks expert review: missing records found late
Expert review slows down when missing records are discovered after the expert has already started reading.
In malpractice cases, missing records are not small annoyances. A chart can appear complete until one missing operative note, nursing flow sheet, imaging report, outside consult, pathology report, or discharge instruction changes the sequence the expert has to evaluate.
The medical narrative summary should help catch these problems early.
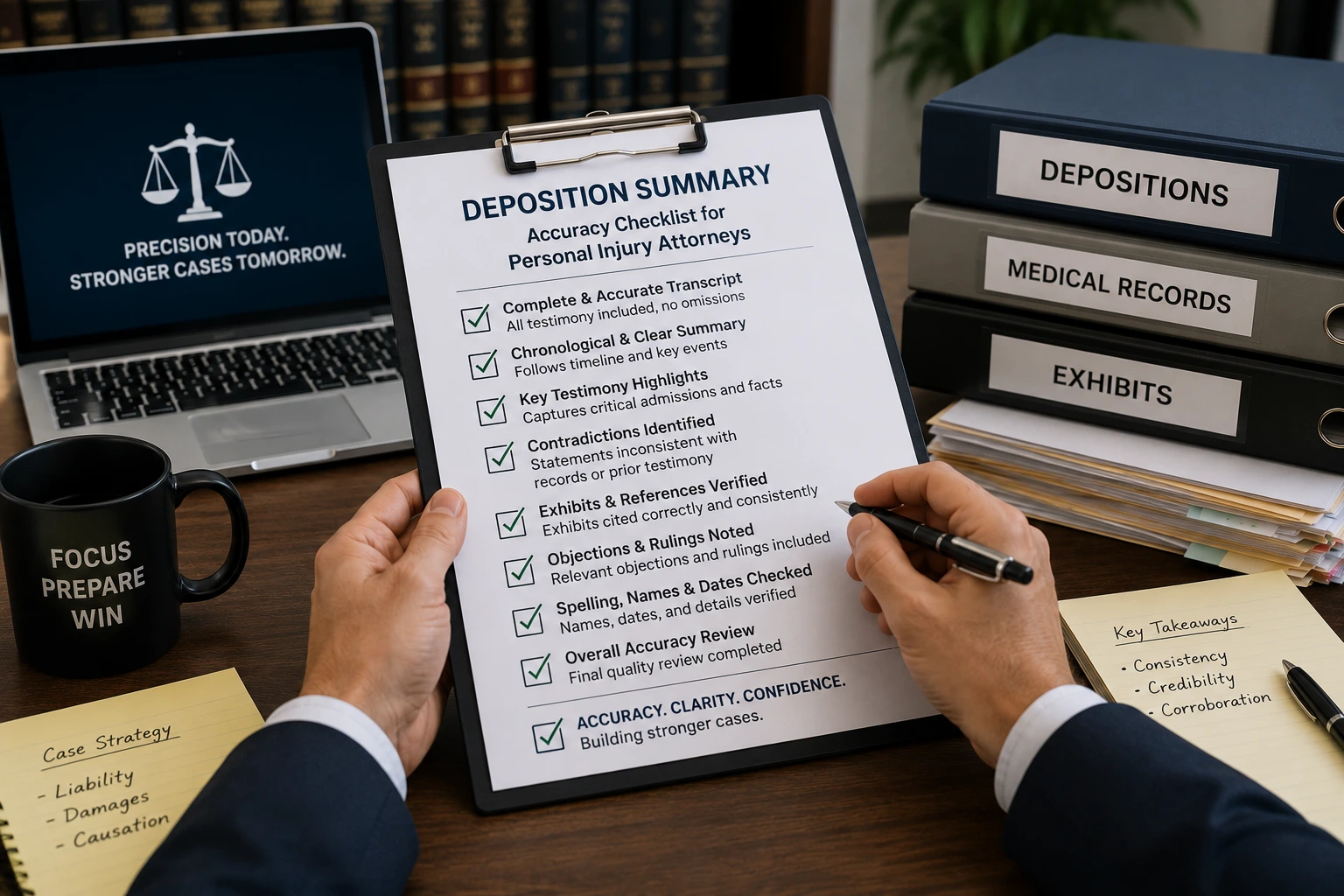
Here is what to check before sending the file:
- Are all provider records included for the relevant date range?
- Does the chart mention outside providers whose records are missing?
- Are diagnostic studies included, or only referenced in progress notes?
- Are medication administration records available when medication timing matters?
- Are nursing notes and flowsheets included when monitoring is part of the review?
- Are consent forms, operative reports, and pathology records present where relevant?
- Are follow-up records included after discharge or transfer?
- Are duplicate records hiding gaps by making the file look larger than it is?
The expert should not have to discover these issues by accident. The attorney should know what is missing before the review clock starts.
A medical narrative summary should prepare the expert to review the record, not force the expert to rebuild it first.
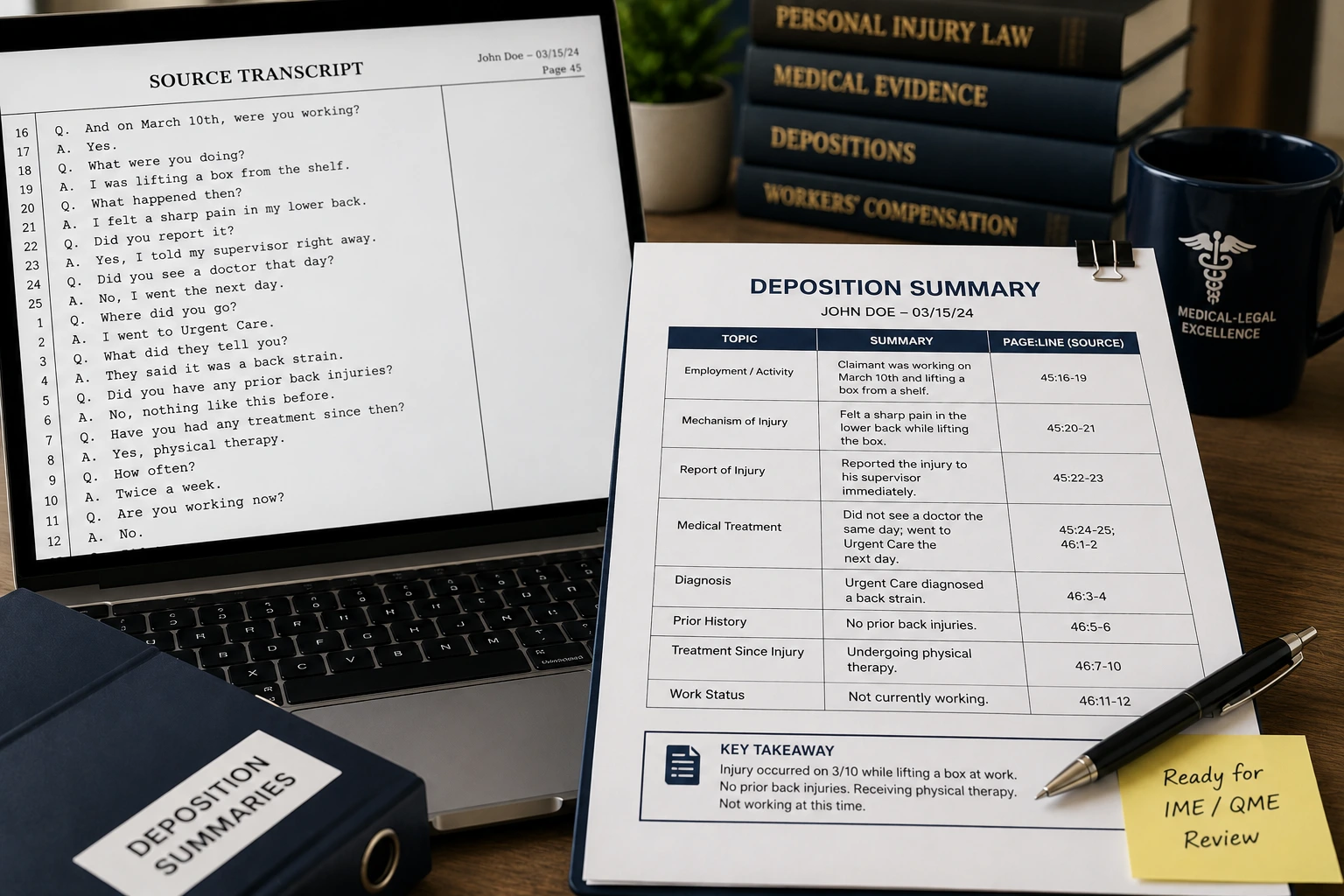
What the medical narrative summary should include
An expert-ready medical narrative summary should tell the treatment story in a way that remains anchored to the records.
For medical malpractice attorneys, that usually means the summary should include the clinical sequence, major provider interactions, key symptoms, diagnostic steps, treatment decisions, changes in condition, procedures, medication events, discharge planning, follow-up care, and documented gaps.
It should also show where the record is unclear.
Useful sections often include:
- Relevant medical background: documented prior conditions, surgeries, medications, allergies, and baseline status when relevant to the expert's review.
- Presentation and initial assessment: symptoms, vital signs, initial exam findings, triage notes, and early diagnostic workup.
- Treatment timeline: provider encounters, orders, tests, procedures, medication administration, and changes in condition.
- Diagnostic record trail: imaging, lab findings, pathology, consults, and reports referenced elsewhere in the chart.
- Care transitions: admission, transfer, discharge, referrals, and follow-up instructions.
- Gaps and inconsistencies: missing reports, conflicting histories, unclear dates, absent follow-up records, or documentation that needs expert attention.
- Source references: page, file, provider, date, and document type where available.
One published LezDo TechMed case study involved a Georgia law firm handling a complex wrongful-death matter with a detailed medical history. LezDo TechMed's role was to organize and cross-reference documented medical information for attorney review. Any conclusions about causation, negligence, or the professional standard remained with the firm's attorneys and retained experts.
That boundary is important. A medical narrative summary can organize the map. The expert still drives the opinion.
Record Preparation Signals Before Expert Review
3 layers
Quality Control
LezDo TechMed deliverables pass through a three-layer quality-control process
2 to 3 days
Narrative Deliverables
General range for medical narrative summary deliverables after scope confirmation
13+ years
Medical-Legal Experience
LezDo TechMed's published medical-legal experience, consistent with its 2013 founding year
Frequently Asked Questions
How does a medical narrative summary help medical malpractice attorneys?

A medical narrative summary helps medical malpractice attorneys prepare records for expert review by organizing the clinical timeline and flagging missing or inconsistent documentation.
What should attorneys check before sending records to a medical expert?
Attorneys should check whether the file includes key provider records, diagnostic reports, operative notes, medication records, nursing documentation, consent forms, discharge records, and follow-up records.
Is a medical narrative summary different from a medical chronology?
Yes. A medical chronology presents events in date order, while a medical narrative summary explains the treatment story in paragraph form. For expert review, attorneys may use one or both depending on the case and the expert's preference.
What makes a medical narrative summary expert-ready?
An expert-ready medical narrative summary is complete, source-supported, clinically clear, and honest about record gaps. It helps the expert understand the documented sequence without forcing them to reconstruct the file from scratch.
To sum up,
Before expert record review, medical malpractice attorneys should follow one practical rule: make the record usable before asking the expert to evaluate it.
A medical narrative summary can help by organizing the treatment story, separating providers and dates, identifying missing records, and giving the expert a source-supported path through the chart. It should not argue the case. It should not give a medical or legal opinion. It should make the documented record easier to examine.
That is where expert preparation becomes cleaner.
The expert can spend more time on the professional review and less time asking where the discharge summary, operative report, medication record, or outside consult went.
Start with the record. The opinion work comes after.
Source Credit : All metrics derived from LezDo TechMed’s internal project data.
Jebisha Jenishofen
Jebisha Jenishofen is a Certified Legal Nurse Consultant and Medical–Legal Research Analyst with over five years of experience in the medical-legal industry. She specializes in medical record analysis, medical-legal research, and content development, creating clear and informative resources on personal injury, medical malpractice, insurance claims, and healthcare litigation. By combining clinical knowledge with research expertise, she transforms complex medical information into practical insights for medical-legal professionals.