Plaintiff and Defense Attorneys Review the Same Records Completely Differently — Here Is Why That Matters
The same medical record can either increase claim value or reduce exposure — depending on who is reviewing it.
Consider this: you hand two attorneys the exact same stack of medical records. Same pages, same dates, same diagnoses, same physician notes, and same imaging reports.
Do you think both attorneys will see the story in the same way? Not at all.
One attorney sees a story of severe injury, ongoing pain, and long-term impact. The other sees treatment gaps, pre-existing conditions, inconsistencies, and signs that the claimant may have recovered earlier than reported.
Same records, but completely different conclusions. Neither side is necessarily wrong.
Experienced plaintiff and defense attorneys are trained to read medical records differently. They look for different patterns, different risks, and different opportunities inside the same documentation.
For insurers, this matters far more than many realize. Because the way medical records are interpreted can directly influence claim value, settlement strategy, reserve decisions, and overall case exposure.
A single overlooked provider note or one undocumented treatment gap can quietly shift an entire claim's direction — and its value. To understand why this happens, insurers first need to understand one important reality about medical documentation.
2X Stronger Chronology Clarity
Integrated medical timelines help claims teams identify narrative gaps and exposure risks hidden across multiple providers.
Medical Records Are Not Objective Truth
Many claims professionals treat medical records as straightforward facts. Collect the records, summarize them, file them, and move forward.
But experienced litigators understand something important.
Medical records are clinical snapshots — not objective truth. They are created under time pressure, shaped by EHR copy-forward templates, influenced by provider assumptions, and often affected by billing requirements.
A physician seeing thirty patients a day is not drafting a legal argument. They are documenting enough information to treat the patient and move forward.
This creates significant room for interpretation — and both sides of litigation know how to use it. Such interpretive flexibility is why the same records can support completely different legal narratives.
What plaintiff counsel sees as evidence of injury, defense counsel may view as inconsistency or unrelated degeneration.
The records may stay the same — but the interpretation surrounding them can significantly affect claim value and litigation strategy.
To understand why, it helps to first examine how plaintiff attorneys review medical records.
Plaintiff counsel is not simply searching for injuries. They are building a causation narrative — a clear connection between the incident and every claimed harm.
Everything before the loss date becomes the baseline. Everything after becomes evidence of impact.
Pre-existing conditions do not disappear from this framework. Instead, they are often presented as aggravated conditions, which may still be compensable in many jurisdictions.
What Plaintiff Counsel Specifically Looks For
The Highest Level of Pain and Limitation
Plaintiff attorneys focus on the highest documented pain scores, the most restrictive functional limitations, and provider notes describing difficulty with daily activities.
Those details often become the foundation of the damages narrative.
Treatment Gaps Reframed as Human Circumstances
Plaintiff counsel may explain treatment gaps through real-life circumstances:
Inability to afford co-pays
Childcare responsibilities
Pressure to return to work despite pain
In that context, the treatment gap becomes humanizing evidence rather than a credibility concern.
Future Care Language
Phrases such as:
“May require further intervention”
“Surgical candidacy to be evaluated”
“Ongoing pain management recommended”
can become the foundation for life care plan claims involving substantial future medical costs.
Even one cautious sentence from a provider can carry significant financial weight once it becomes part of litigation strategy.
The same records, however, can support a very different interpretation when viewed from defense perspective.
How Defense Attorneys Review the Exact Same Records
Defense counsel performs an equally detailed — but completely opposite — review of the same documentation.
Where Defense Review Begins
Before reviewing post-incident treatment, defense attorneys often map the claimant’s pre-existing medical history first.
That includes:
Prior workers’ compensation claims
Chronic pain documented before the incident
Earlier imaging showing degenerative findings
Each detail may support an alternative causation argument or an apportionment position that directly affects damages exposure.
What Defense Counsel Specifically Looks For
Objective Findings Versus Subjective Complaints
When a claimant consistently reports severe pain but imaging shows only mild age-related findings, defense counsel may view that mismatch as both a credibility concern and a causation issue.
Treatment Gaps Interpreted Differently
Where plaintiff counsel sees life circumstances, defense counsel may see evidence that the injury was not severely disabling.
Serious debilitating injuries generally produce consistent treatment-seeking behavior.
Litigation Timeline Patterns
If treatment intensity noticeably increases after an attorney is retained, experienced defense reviewers document that pattern carefully.
The records themselves do not change. The interpretation does.
The contrast becomes even clearer when both sides interpret the exact same treatment timeline differently.
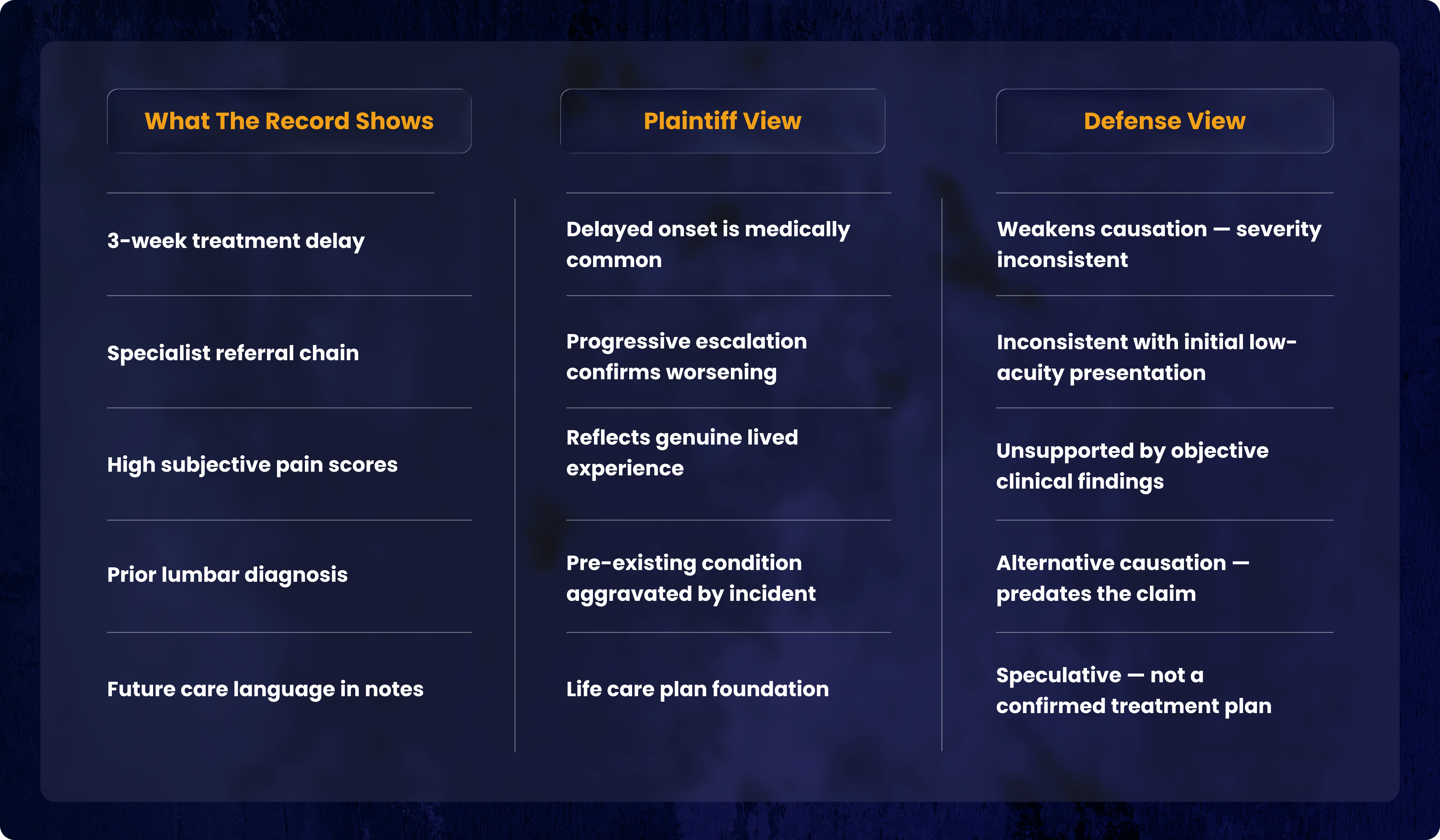
The Same Record — Two Completely Different Arguments
Consider one common scenario: a claimant delays treatment for three weeks after the incident.
The exact same documentation can support two very different narratives depending on how the records are interpreted during litigation.
Five identical facts. Five completely different arguments.
This happens in significant claims every day.
The records themselves may never change — but the interpretation surrounding those records can dramatically affect reserve exposure, settlement strategy, and overall claim valuation.
Where Claim Exposure Quietly Expands
The most expensive failures in claims analysis rarely happen suddenly.
They build gradually — small interpretive gaps that compound into significant financial exposure over time.
Fragmented Provider Review
When records from multiple providers are reviewed separately instead of together, important contradictions can be missed.
For example:
A claimant reports full range of motion to one provider during the same week, but they tell another provider they cannot lift their arm past shoulder height.
That inconsistency only becomes visible when all records are reviewed together on an integrated timeline.
Missing What Was Never Documented
If a claimant alleges severe cognitive impairment, but no treating physician documented cognitive complaints or ordered neuropsychological testing, that absence may become a valuable defense point.
But it only helps if someone actively identifies it during review.
Copy-Forward Documentation
When fourteen consecutive chiropractic visits contain nearly identical wording, that may suggest administrative templating rather than genuine clinical progression.
Plaintiff counsel is unlikely to focus on that issue. A thorough review process should be able to detect it.
Chronology Gaps
Missing the fact that a claimant was already receiving pain management treatment before the alleged incident is not a minor oversight.
It is a case-changing detail that can directly affect reserve accuracy, liability exposure, and settlement valuation.
“Integrated record analysis helps uncover contradictions and chronology gaps that siloed review often misses.”
What Strong Claims Teams Are Doing Differently
High-performing claims organizations have stopped asking:
“Do we have the records?”
They are now asking:
What story do these records create?
How would plaintiff counsel present that story?
Where are the causation vulnerabilities?
Where do subjective complaints conflict with objective findings?
What does the integrated timeline reveal that isolated records do not show?
That shift — from collection to analysis, from summary to strategy — changes litigation preparation entirely.
Many insurers have found that specialized medical record review services provide this level of insight at scale. Outsourcing medical record review to experienced litigation support teams can improve claim evaluation before opposing counsel establishes the narrative.
Clearer Claim Insights. Faster Case Review
82%
Improved visibility
Highlights key facts
67%
Time efficiency gain
Speeds review process
91%
Accuracy improvement
Reduces documentation errors
Frequently Asked Questions: Medical Records in Personal Injury Claims
Why do plaintiff and defense attorneys draw different conclusions from the same records?
They review the records with different objectives. Plaintiff attorneys focus on proving injury, impact, and damages, while defense attorneys look for inconsistencies, treatment gaps, and alternative explanations.
Can one provider note really affect claim value that much?
Yes. Even a short provider note can influence how future treatment needs, injury severity, or long-term impact are viewed during litigation.
Are treatment gaps always harmful to a claimant’s case?
Not always. Plaintiff counsel may explain treatment gaps through financial limitations, work responsibilities, or personal circumstances. Context matters.
How do pre-existing conditions affect a personal injury claim?
Pre-existing conditions do not automatically weaken a claim. In many cases, the discussion centers on whether the incident aggravated an existing condition.
Why does copy-forward documentation matter in medical records?
Repeated notes with nearly identical wording may suggest templated documentation rather than meaningful clinical progression, which can raise credibility concerns.
How can medical record interpretation affect reserves?
The way records are interpreted affects perceived claim exposure. Consistent records may support higher reserves, while contradictions and gaps may reduce perceived severity.
What is an integrated medical record review?
It is a review process where all provider records are analyzed together on a single timeline instead of separately, making inconsistencies and missing details easier to identify.
What are common mistakes during medical record review?
Common mistakes include reviewing records in isolation, overlooking missing documentation, and failing to connect events across the full treatment timeline.
Why do subjective complaints and objective findings matter so much?
When reported symptoms do not align with clinical findings, it can raise questions about severity, credibility, and causation.
How should insurers approach medical record review differently?
Strong claims teams focus not only on collecting records, but also on understanding the narrative those records create and how that narrative may be presented during litigation.
The Bottom Line
The challenge for insurers is not choosing between two interpretations of the same records, but making sure neither perspective is incomplete. When medical information is reviewed in isolation, important details can be missed, and decisions may become inconsistent.
This is where a structured, integrated review becomes essential. It brings all records into a single, connected timeline, helping insurers see the full clinical picture clearly and objectively.
The result is more balanced decision-making—grounded in evidence, supported by complete context, and less influenced by how either side presents the case.
Source Credit : All metrics derived from LezDo TechMed’s internal project data.
Shabila Thomas
Shabila T is a Medical–Legal Research Analyst with a strong focus on in-depth research and content development in the medico-legal field. She specializes in analyzing industry trends, regulatory updates, and legal–medical practices to create clear, accurate, and impactful blogs that address key challenges faced by professionals. Her research-driven writing helps medical and legal firms address the industry pain points and boost their business operations.