Home
>
Blog
>
>
Narrative Summary Reports for QMEs: Getting Accuracy and Completeness Right
Before you build an opinion on a narrative summary, here's what accuracy and completeness really require:
- Your report rests on it – a QME opinion is only as sound as the summary it's built on.
- Complete means every provider – prior injuries, treatment gaps, and missing records all flagged, including the ones that are easy to miss.
- Accurate means source-linked – correct dates and providers, each entry traceable to the page, so you can verify without re-reading.
- Prior conditions surfaced, not decided – the summary flags documented prior conditions; you weigh apportionment.
Read on for what accurate and complete really mean, and how to trust a summary before your evaluation.
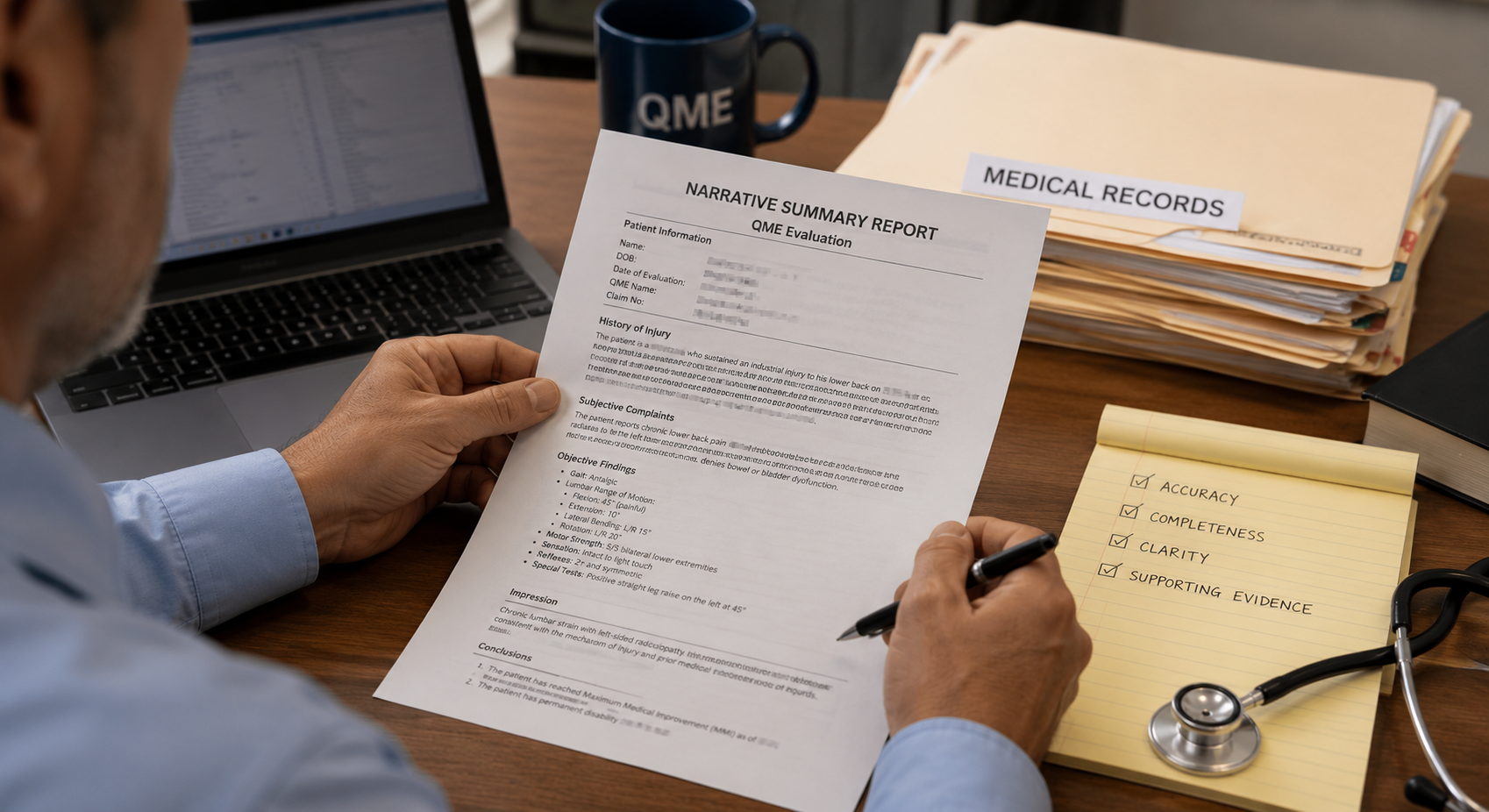
Your QME report is only as sound as the summary it's built on. If a narrative summary misses a prior injury or gets a date wrong, that error doesn't stay in the summary. It walks straight into your opinion. So for a QME, accurate and complete isn't a nice-to-have. It's the whole point. Worried you're relying on a summary you haven't fully checked? Let's talk about what to look for.
Quick level-set: a narrative medical summary is a prose account of the claimant's medical history and treatment, drawn from the records, so you can read the story instead of the raw file. For an evaluation, it's what lets you get to the medical questions faster, but only if you can trust it.
Why accuracy and completeness matter more for a QME
Here's the thing: your opinion gets tested. At deposition, on reconsideration, in cross-examination, the record foundation behind your report is fair game. A summary that quietly dropped a provider or misread a date can turn into a hard question you didn't see coming. Accuracy and completeness aren't about tidiness. They're about defensibility.
Three Layers of Quality Control
Every deliverable passes a three-layer quality-control review by medical and paramedical reviewers, so accuracy and completeness are built into the process rather than inspected in at the end.
What complete really means
Complete is more than every page being here. It means every provider and relevant encounter is accounted for, prior injuries and conditions to the same body part are surfaced, treatment gaps are visible, and anything missing is flagged so you can request it before the eval. A summary that reads smoothly but skips a provider isn't complete. It only looks complete, and the gap is where a QME opinion gets exposed.
What accurate really means
Accurate means the details hold up: correct dates, correct providers, entries anchored to the records rather than loosely paraphrased, and duplicates removed so the treatment course isn't overstated. The test is simple. Can you trace any statement back to the source page and confirm it? If you can, you can rely on it. If you can't, you're back to re-reading the file.
Want a summary you can trust before your next eval?
Prior conditions, apportionment, and the line the summary won't cross
This is where accuracy and boundaries meet. A good narrative summary surfaces documented prior injuries and pre-existing conditions and points you to the source, because those change how the current record reads. What it doesn't do is decide apportionment, causation, or impairment. That's your call. The summary organizes and flags the documented evidence, and you weigh what it means. Keeping that line clean is part of what makes the summary safe to rely on.
How to trust the summary without re-checking it
The fastest way to trust a summary is to be able to verify it in seconds. Source or Bates references on every entry let you jump to the page and confirm a date, a diagnosis, or a provider without re-reading the whole file. If a summary can't point you back to the record, you'll end up re-doing the work, which defeats the purpose.
A narrative summary is only as good as your ability to verify it. Source-linked accuracy is what makes it usable.
How to judge a narrative summary's accuracy and completeness
A quick gut-check before you rely on one: Are all the providers and key encounters here, and are gaps flagged? Can you trace any statement to a source page? Are prior conditions surfaced without being interpreted for you? Is there a human review step behind any AI-assisted extraction? If the answers are yes, you've got a summary you can build an opinion on. If not, you've got more reading to do.
What Accuracy and Completeness Look Like
Every Provider
Complete
All providers, encounters, and prior conditions accounted for, with gaps flagged
Source-Linked
Verifiable
Each entry traceable to the record, so you can check it in seconds
3-Layer QC
Reviewed
Medical and paramedical reviewers verify before it reaches you
QME Narrative Summary FAQs
What is a narrative summary report for a QME?

A prose account of the claimant's medical history and treatment, drawn from the records, so a QME can read the medical story instead of the raw file. For an evaluation, it organizes the documented history, prior conditions, and treatment course with source references.
Why do accuracy and completeness matter so much for a QME summary?
Because your opinion is built on it, and that foundation gets tested at deposition and on reconsideration. A summary that misses a provider or misstates a date can weaken an otherwise sound report. Accuracy and completeness are about defensibility, not tidiness.
What makes a narrative summary complete?
Every provider and relevant encounter accounted for, prior injuries and conditions surfaced, treatment gaps visible, and missing records flagged so you can request them before the eval. A summary that skips a provider only looks complete.
How can I trust a summary without re-reading the records?
Look for source or Bates references on every entry. If you can trace any statement back to the page in seconds, you can rely on it. If it can't point you to the record, you'll end up re-checking it yourself.
Does a narrative summary decide apportionment or causation?
No. It surfaces and flags documented prior conditions, gaps, and inconsistencies, and points to the source. Apportionment, causation, and impairment are the QME's determinations, not the summary's.
Does AI write the narrative summary?
LezDo TechMed uses a human-in-the-loop model: AI-assisted extraction and indexing handle the first pass, and a medical or paramedical reviewer verifies for context, accuracy, and completeness. No honest process claims 100% accuracy.
How do I know a summary is accurate before I rely on it?
Check that providers and encounters are complete with gaps flagged, that entries are source-linked, that prior conditions are surfaced without interpretation, and that a human verified any AI-assisted output. Those four checks tell you whether it's ready to build an opinion on.
The bottom line
For a QME, a narrative summary is the foundation your opinion stands on, so accuracy and completeness aren't optional. A summary that's complete, source-linked, and human-verified lets you spend your time on the medical judgment instead of checking someone else's work. That's the difference between a summary you read and a summary you can rely on.
Source Credit : All metrics derived from LezDo TechMed’s internal project data.
Anjana Devi Vijay
Anjana Devi Vijay is a Certified Legal Nurse Consultant (CLNC) and Medical–Legal Research Analyst with 9+ years of experience in medical record review, deposition summary analysis, and medico-legal research. She specializes in transforming complex healthcare documentation into accurate, actionable insights that support attorneys, insurers, and medical evaluators. With expertise in clinical documentation analysis and legal case support, she creates research-driven content focused on improving decision-making and case outcomes.



.webp)
.webp)