Home
>
Blog
>
>
Medical Chronology for Nursing Home Abuse Cases — What the Timeline Must Capture
A clear medical chronology connects scattered nursing home records into one timeline—making neglect, delays, and care failures easier to identify.
Nursing home abuse happens more often than most people realize. Many elderly residents go through neglect, poor care, or physical harm every single day. And in most of these cases, the warning signs were sitting right there in the medical records — but nobody put them together.
That is exactly what a medical chronology does.
It takes all the scattered records — nursing notes, hospital files, lab reports, medication logs — and arranges them in date order. Suddenly, the full picture becomes clear. What happened. When it happened. What the nursing home did about it. And what they failed to do.
For IME and QME professionals, a good medical chronology means faster reviews, stronger expert opinions, and testimony you can stand behind confidently. For attorneys, it turns thousands of confusing pages into a story anyone can follow.
Understanding Medical Chronology in Nursing Home Abuse Cases
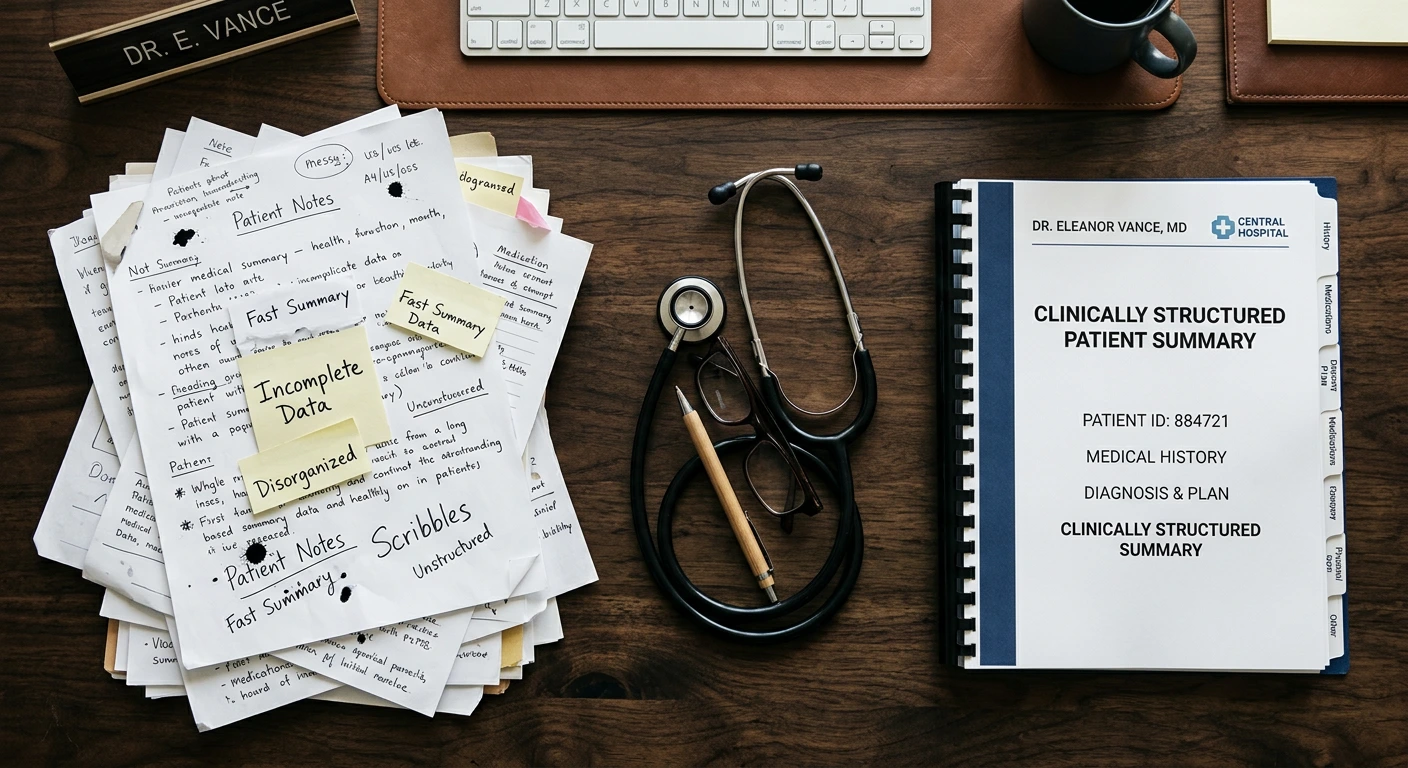
A medical chronology is a structured timeline. It organizes all the important medical events in a case — in the order they actually happened.
Instead of reviewing thousands of confusing pages, they get one clear document that explains the case from start to finish.
In nursing home cases, a good chronology does three things:
- Puts every medical event in the correct date order
- Pulls from all record sources — nursing notes, doctor orders, hospital files, medication records
- Presents complex medical information in simple language anyone can understand
Why It Matters in Abuse and Neglect Cases
Nursing home neglect does not happen all at once. It happens slowly over time. A missed dose, an untreated wound, or a fall with no follow-up may seem small. But when they add up, they show a bigger problem.
A medical chronology connects these events and helps:
- Spot neglect — Shows exactly when proper care stopped and what happened as a result
- Track health changes — Makes it visible how the resident's condition got worse over time
- Support the case — Gives attorneys and IME/QME experts solid, documented facts to work from
Review Cases 60% Faster
When the medical chronology is already organized, IME and QME professionals spend less time on records — and more time on the expert opinion that wins the case.
Why Nursing Home Abuse Cases Need Detailed Timelines
Elderly patient records are more complex than they look.
Nursing home residents usually have more than one health problem. Many deal with conditions like diabetes, heart disease, dementia, or difficulty moving — all at the same time. On top of that, most of them have years of medical history from different doctors and hospitals before they even entered the facility.
Because of this, reviewing nursing home abuse cases can quickly become complicated. Medical records often come from multiple sources, including:
- Nursing homes
- Hospitals and emergency rooms
- Primary care physicians
- Specialists
- Rehabilitation centers
Without a clear timeline, it becomes hard to tell which problems were caused by the nursing home and which ones the resident already had before admission.
Here is what IME and QME professionals should capture in the timeline.
Ready to get started? Get free trial worth $500. Hurry up!
What Every IME and QME Professional Must Capture from Medical Chronology
1. The Resident's Starting Health Condition
As an IME or QME reviewer, your evaluation starts here. The admission records are your baseline — your “before” picture. Without this, it becomes difficult to separate pre-existing conditions from problems caused by the nursing home.
- Admission records — What diagnoses, medications, and physical condition did the resident arrive with?
- Existing illnesses — What health problems already existed before the facility’s care began?
- Mobility and mental condition — Could the resident walk? Were they mentally alert and aware?
- Baseline health status — Weight, skin condition, and vital signs on admission
Without a clear baseline — forming a strong causation opinion becomes much harder.
2. Injuries and Medical Incidents
Every injury should appear in the timeline with complete context. For IME and QME professionals, these details help determine whether proper care was provided after the incident.
- Falls — Date, location, who was present, and what the facility did afterward
- Fractures — When they were identified and whether there was any delay in diagnosis
- Bruises — Location, appearance, and whether the explanation matches the injury pattern
- Head injuries — Even minor injuries should be documented carefully
- Emergency treatment — What treatment was given and how quickly staff responded
3. Pressure Ulcers and Wound Progression
For IME and QME evaluations, wound progression is some of the clearest evidence in a nursing home abuse case. It shows whether proper preventive care was actually provided.
The timeline should track:
- When the wound was first noticed and its initial condition
- How the wound progressed over time — Stage 1, 2, 3, or 4
- Whether infection developed during the resident’s stay
- Whether wound care was ordered and properly carried out
A bedsore that worsens from Stage 1 to Stage 4 during the resident’s stay may show serious failures in care and monitoring.
4. Medication and Treatment History
The MAR — Medication Administration Record — is one of the most important records IME and QME professionals review. It shows whether medications were given correctly and consistently.
- Medication changes — Additions, removals, dose changes, and the reasons behind them
- Missed doses — How often medications were skipped and the impact on the resident
- Wrong medications — Incorrect drug, dose, or administration method
- Adverse reactions — Medical complications that followed medication changes
The chronology should give special attention to sedatives or anti-psychotic medications used without a proper diagnosis, as this may indicate chemical restraint or abuse.
“Medical chronologies turn confusing nursing home records into a clear timeline of care, neglect, and outcomes.”
5. Delays in Medical Care
This section often provides some of the strongest support for causation findings. Delayed care can directly connect facility failures to worsening injuries or medical decline.
- Delayed doctor notification — Symptoms documented but not reported promptly
- Delayed hospital transfer — The resident’s condition worsened before emergency care was provided
- Untreated symptoms — Pain, fever, or breathing issues recorded without follow-up treatment
- Missed follow-ups — Ordered tests or specialist visits that never occurred
These delays can turn manageable conditions into serious or life-threatening situations.
6. Physical and Mental Decline
A strong chronology should also capture the resident’s overall decline during their stay. This helps IME and QME professionals evaluate long-term impact and quality-of-life changes.
- Ongoing weight loss without intervention
- Repeated lab findings showing dehydration or malnutrition
- A mentally alert resident becoming confused or withdrawn
- Fear, anxiety, or behavioral changes that developed during the stay
When viewed together, these patterns often reveal neglect more clearly than any single incident.
7. Hospital Visits and Emergency Transfers
Hospital records are especially valuable because they are independent from the nursing home’s documentation. For IME and QME reviewers, they often provide a clearer picture of the resident’s actual condition.
- ER visits — Why the resident was sent and what the hospital found
- Diagnostic findings — Hospital diagnoses that conflict with facility records
- Specialist notes — Conditions the nursing home should have identified earlier
- Repeated admissions — Multiple hospitalizations for the same issue may point to ongoing care failures
8. Documentation Gaps and Inconsistencies
For IME and QME professionals, missing or inconsistent documentation can become critical evidence. These gaps should always be highlighted clearly in chronology.
- Days with no nursing notes for a critically ill resident
- Nursing notes describing the resident as “stable” while hospital records show severe illness
- Care plans requiring repositioning with no documentation proving it happened
- Multiple notes entered together after a serious incident, suggesting delayed charting
In many nursing home abuse cases, these documentation gaps are not minor issues — they are central to the expert evaluation.
How Medical Chronologies Strengthen Nursing Home Abuse Cases
55%
Faster Case Understanding
Organized timelines simplify thousands of pages of nursing home records
45%
Better Neglect Identification
Chronologies expose treatment delays, documentation gaps, and care failures
50%
Stronger Expert Support
Clear medical timelines help IME/QME professionals build defensible opinions
FAQs About Medical Chronology in Nursing Home Abuse Cases
What is medical chronology in a nursing home abuse case?

It is a timeline that puts all medical events in date order. It turns scattered records into one simple, easy-to-read document.
Why is medical chronology important in nursing home abuse cases?
Neglect builds up slowly over time. A chronology connects all the small signs together and shows the full picture of what went wrong.
What makes a good medical chronology?
It must be accurate, complete, easy to follow and organized clearly in date order. It should summarize important medical events without leaving out critical details or documentation gaps.
What records are included in a nursing home medical chronology?
Nursing notes, doctor orders, medication logs, hospital records, lab results, and incident reports.
How does a medical chronology help IME and QME professionals?
It saves time, makes key injuries easy to find, and helps experts build strong, well-supported opinions.
What are the most common signs of nursing home neglect found in medical records?
Repeated falls, worsening bedsores, medication mistakes, unexplained bruising, weight loss, and repeated hospital visits.
Why are documentation gaps important in nursing home abuse cases?
Because missing records and inconsistencies are often the strongest evidence in the case.
What is the MAR and why does it matter?
The MAR is the Medication Administration Record. It shows whether the resident actually received the medications the doctor ordered.
How do hospital records help in a nursing home abuse case?
They are independent records that often reveal what the nursing home failed to document or left out in their own notes.
Can a medical chronology help prove nursing home negligence?
Yes. It reveals patterns of neglect and treatment failures — and gives attorneys and IME and QME professionals the facts they need to build a strong case.
How Medical Chronologies Support IME and QME Evaluations
Faster and Clearer Record Review
IME and QME professionals often work under tight deadlines with large volumes of records. A well-organized chronology cuts through that volume and saves significant time.
- The case is easier to understand from the start
- Key injuries and health changes are easy to find
- Patterns and red flags are visible right away
- More time can be spent forming the expert opinion rather than hunting through records
Supporting Expert Opinions on Causation
The chronology is also the backbone of the causation opinion — the part that directly links the facility's failures to the resident's harm.
- Points to specific dates and specific failures — not vague statements
- Shows clearly how an injury developed and worsened over time
- Helps assess how the resident's quality of life was affected over the long term
- Makes the expert opinion more defensible under cross-examination
Final Thoughts
Nursing home residents are some of the most vulnerable people in our society. Many of them cannot speak up for themselves. The medical records are often the only voice they have.
A thorough medical chronology makes sure that voice is heard. It shows the full story — clearly, honestly, and in a way that leaves nothing hidden.
Build it carefully. Keep it complete. And let the records tell the full truth.
Source Credit : All metrics derived from LezDo TechMed’s internal project data.
Vishnu Priya Vinu
Vishnu Priya Vinu is a Medical-Legal Research Analyst with over two years of experience in medical record review, medico-legal research, and content development. She specializes in blogs, articles and E-books that bridges the gap between healthcare and law. Her strong medical background brings depth and accuracy to content, enabling law firms, medical evaluators, and insurance professionals to gain insights on complex medical data analysis. She delivers evidence-based insights and strategic content that strengthen case outcomes and support informed decision-making.